Published May 29, 2026
8 minute read
Most women considering breast augmentation arrive at their consultation with a question written down. But, and I see this all the itme, underneath that question is usually a fear they haven't said out loud yet — about pain, about safety, about whether they'll still look like themselves, about whether anyone will be able to tell.
After performing thousands of breast implant procedures and a career rooted in reconstructive surgery — rebuilding breasts after cancer, trauma, and congenital differences — I've heard nearly every concern a patient can have. Some are based on outdated information. Some are entirely valid. All of them deserve a straight answer.
Here are the fears patients raise most often in my Northwest Arkansas consultations, and what the honest answers actually are.
"Will my implants look fake?"
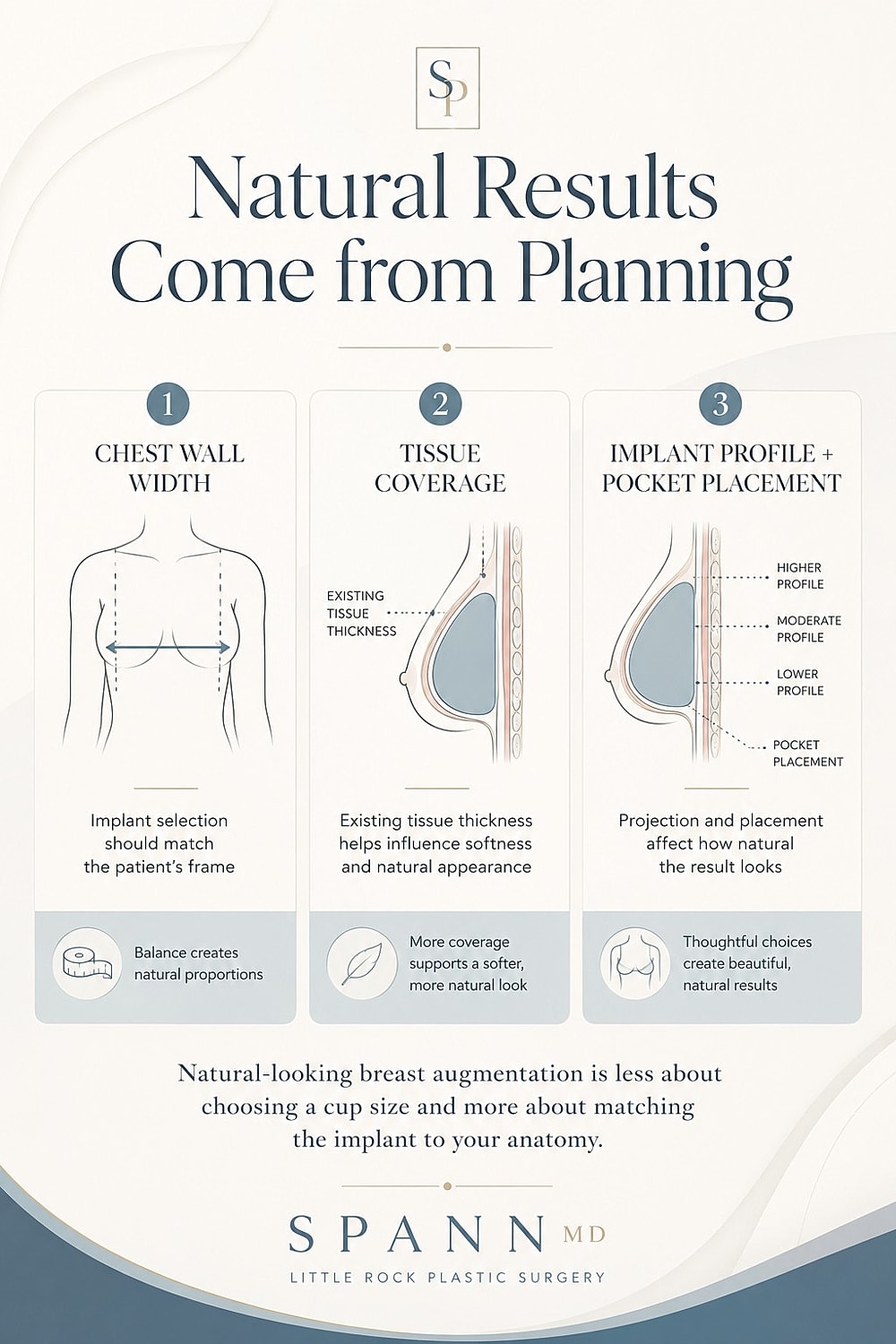
This is the number one fear, and the answer depends almost entirely on three decisions made before surgery: implant size, implant profile, and pocket placement.
I'm a big believer in natural. Implants look obvious when they're too large for the chest wall they're sitting on, when the profile is too projecting for the patient's frame, or when they're placed too high or too tight. None of these are inevitable. They're planning failures. A well-planned augmentation works with your existing anatomy — your chest width, your tissue thickness, your nipple position, your natural breast slope. When the implant matches the patient instead of the patient adapting to the implant, the result reads as a natural, fuller version of the breasts you already have. People notice that you look great. They don't notice surgery. In consultation, we measure the chest wall, assess tissue coverage, and discuss profile options before any size is selected. Sizing is the last decision, not the first.
"How much pain should I expect?"
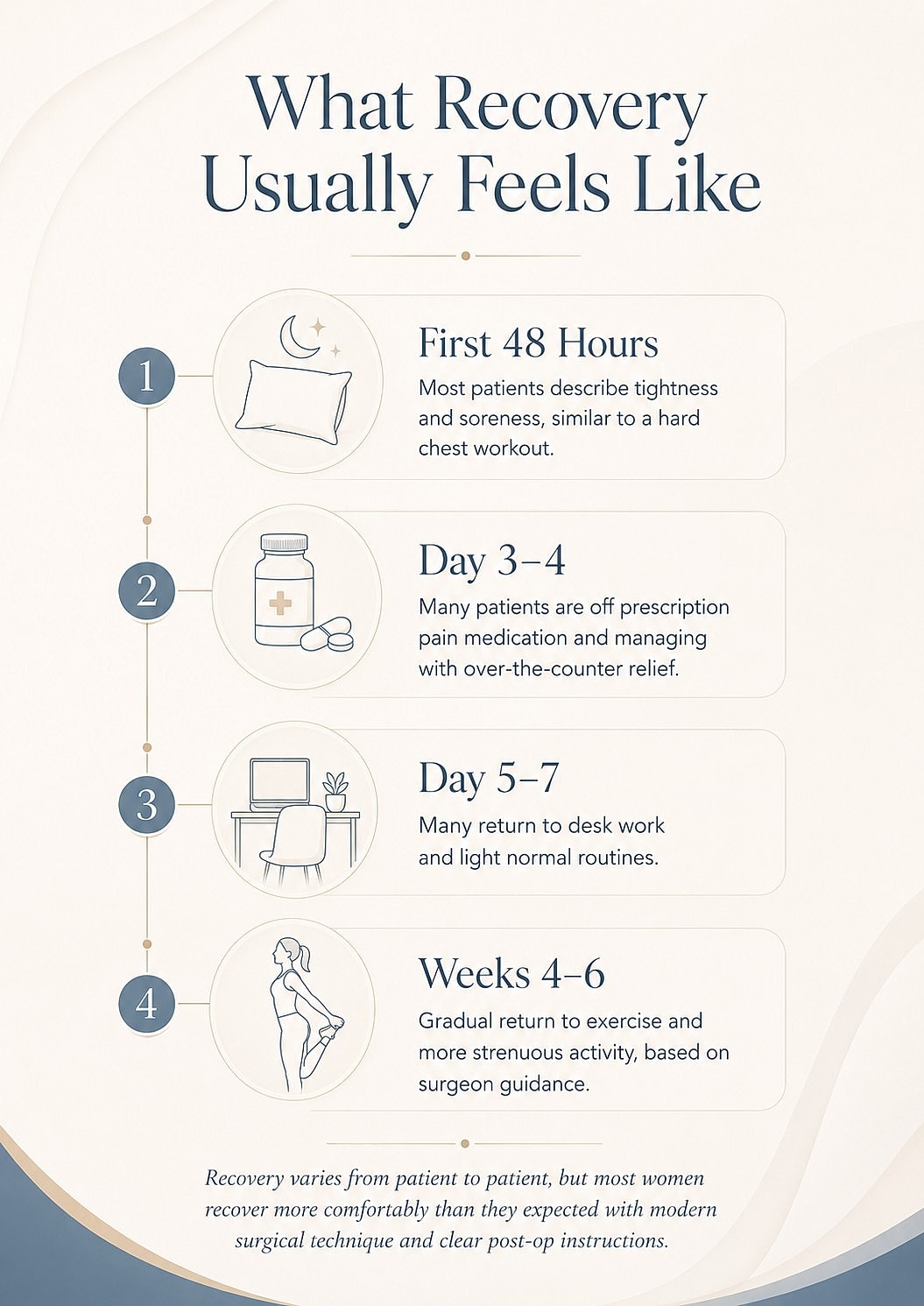
Less than you've probably been told. Recovery from breast augmentation has changed substantially in the last decade.
Most patients describe the first 48 hours as soreness and tightness — similar to a hard chest workout — rather than sharp pain. By day three to four, most patients are off prescription medication and managing with over-the-counter pain relief. Many return to desk work within five to seven days.
Several factors keep modern recovery comfortable: meticulous surgical technique that minimizes tissue trauma, long-acting local anesthetic placed at the time of surgery, multi-modal pain management (combining several non-narcotic medications), and clear instructions on movement during the first week. Patients who follow the post-op protocol almost always do better than they expected.
The patients who struggle with recovery are usually the ones who tried to "push through" early — lifting children, returning to workouts, driving on day two. The protocol exists for a reason.
That said, Motiva Preserve shortens the rapid recovery by about half.. So essentially back to work in 1 day. Moderate exercise at a week.
"Are silicone implants safe? What about Breast Implant Illness?"
This concern is real, and it deserves a real answer rather than dismissal.
Modern silicone implants are the most studied medical device in the FDA's history. The cohesive silicone gel used today is fundamentally different from the liquid silicone implants of the 1980s and 1990s — it holds its shape even when cut, similar in consistency to a gummy candy.
Breast Implant Illness (BII) is the term patients use to describe a constellation of systemic symptoms — fatigue, brain fog, joint pain, autoimmune-like complaints — that some women attribute to their implants. The medical literature has not established a causal mechanism, but a meaningful subset of patients report symptom improvement after implant removal. I take this seriously. It is part of every consultation I have.
What I tell patients honestly: the overwhelming majority of women with breast implants do not develop systemic symptoms. But you have the right to know that BII is a real reported phenomenon, that the cause is not fully understood, and that explant surgery is an option if you ever change your mind. Anyone who tells you implants are 100% risk-free is selling you something. Anyone who tells you they're certainly dangerous is doing the same thing from the opposite direction.
"Will I lose nipple sensation?"
Temporary changes in nipple sensation are common in the first few months — usually heightened sensitivity, occasionally numbness. The vast majority of patients return to normal sensation within six to twelve months.
Permanent significant sensation loss is uncommon and is influenced by incision choice, implant size relative to the breast, and surgical technique. Larger implants placed through certain incisions carry slightly higher risk. This is discussed and planned around during consultation, particularly for patients for whom nipple sensation is a high priority.
"Can I still breastfeed?"
In most cases, yes. The milk-producing structures of the breast are largely preserved with the incision and pocket techniques used in modern breast augmentation. Studies of post-augmentation breastfeeding show that the majority of patients who attempt to breastfeed are able to do so, though some women — augmented or not — have lower milk supply for unrelated reasons.
If breastfeeding a future child is important to you, tell your surgeon. It affects the incision recommendation.
"What if I hate them?"
This is the fear patients are often most embarrassed to bring up, and it's one of the most important to address directly.
The honest answer: a small percentage of patients want a change after their initial surgery. Sometimes that's a size adjustment, sometimes it's a profile change, sometimes it's something they couldn't have anticipated until they lived with the result for a few months.
This is one of the reasons the consultation process matters so much. We use sizing systems, before-and-after galleries of patients with similar anatomy, and detailed conversations about lifestyle — do you run, lift, wear fitted clothing, prefer a sports-bra silhouette or a fuller look in a dress? — to align expectations before the operating room, not after.
Revision surgery exists, and good surgeons plan for the possibility from the first consult. But the goal is to get it right the first time, and that starts with not rushing the decision.
"How long do implants last? Will I need surgery again?"
Implants are not lifetime devices. The current realistic expectation is that most patients will have at least one additional procedure over the course of their lifetime — whether for an implant exchange, a size change after pregnancy or weight changes, a lift to address natural tissue settling, or eventual removal.
This is not a reason to avoid augmentation. It's a reason to choose a surgeon and a practice you trust to be there for the long arc, not just the first surgery.
"Will surgery be safe? What about the surgery center itself?"
The facility matters as much as the surgeon. Our procedures are performed in an AAAASF-accredited surgical facility — the same accreditation standard used by hospital-based outpatient centers — with board-certified anesthesia, full emergency protocols, and the equipment and staffing to handle the rare complication safely.
Cost-shopping a cosmetic procedure into a non-accredited facility is one of the few decisions in cosmetic surgery that can genuinely harm you. The right questions to ask any surgeon: Is the facility accredited, and by whom? Who provides anesthesia, and what are their credentials? What is your complication rate, and what is your plan if one occurs?
"How do I know I'm choosing the right surgeon?"
Look at three things:
Training and credentials. Board certification in plastic surgery by the American Board of Plastic Surgery is the baseline, not the ceiling. Beyond that, what does the surgeon do day in and day out? A reconstructive background — rebuilding breasts after mastectomy, treating complex revisions, managing complications — sharpens the judgment that aesthetic-only practices sometimes lack.
Volume and consistency. Ask how many breast augmentations the surgeon performs annually, and ask to see results from patients who started where you're starting. Not the surgeon's best result. A patient like you.
The consultation itself. A good consultation is a conversation, not a sales pitch. You should leave understanding what's recommended for your anatomy and why — not just what's on the menu.
The Real Question Underneath All the Others
Most patients aren't really asking "will it hurt" or "will it look fake." They're asking can I trust this process, and can I trust the person doing it?
That's the right question. The answers come from honest information, time spent in consultation, and a surgeon willing to tell you when augmentation isn't the right choice — because sometimes it isn't, and saying so is part of the job.
If you're considering breast augmentation in Northwest Arkansas and want a consultation that addresses the real questions — not just the easy ones — we'd be glad to meet you.